FAQ UTI
Answers to all questions about urinary tract infections
Antibiotics
Suitable antibiotics help well, but are not always necessary.
In the case of an uncomplicated bladder inflammation, the spontaneous healing rate is reportedly around 30-50% after a week according to studies (after one week, 30-50% of all acute, uncomplicated HWI's heal by themselves without antibiotic treatment). This means that at least one-third of all acute, uncomplicated UTIs will resolve on their own without antibiotic treatment.
As a result, the main focus in treating an uncomplicated bladder inflammation is to get the clinical symptoms under control more quickly (e.g. with plant-based medications and pain relief medication like ibuprofen).
When does one speak of an uncomplicated bladder inflammation? The majority of uncomplicated cases are those in which the infection has not spread to other parts of the urinary tract.
Conclusion: A UTI is suitable for self-medication only in uncomplicated cases.
My experience: Online, one often finds that it can take several weeks for a bladder inflammation to heal on its own. If my symptoms and the urine test strip have not improved after 3-5 days of self-medication without AB (antibiotics) have not changed noticeably, I have always ended up taking antibiotics.
My tip in case of first signs of a UTI: Go to the doctor and get your urine tested, and have it sent for culture and sensitivity testing. If you still try to tackle the problem with natural remedies after a few days, that's fine! But if not, then at least you will have an antibiotic treatment plan with the list of susceptible antibiotics for your bacteria (your germs) ready.
Until just a few years ago, antibiotics were the standard therapy for bladder infections, even for uncomplicated ones. I can confirm this from personal experience.
However, it is now known that the uncritical use of antibiotics is a serious mistake – even though the quick relief of symptoms through antibiotic use is very tempting.
Warning: Resistance Development: When antibiotics are taken indiscriminately and are also used extensively in livestock farming, resistance development increases. Infections with (multi)resistant bacteria are often severe and sometimes even incurable. In the EU, more than 30,000 people die each year from such infections.
Warning: Microbiome: Another reason to question the repeated use of antibiotics is the gut microbiome. Bacteria are not inherently harmful but are, in fact, a necessary component of a healthy organism. The prolonged use of antibiotics can severely impact the gut flora and lead to health problems elsewhere in the body.
Warning: Side Effects: Antibiotics generally have more side effects than phytopharmaceuticals. These range from typical gastrointestinal issues to permanent side effects such as nerve damage with fluoroquinolones (Ciprofloxacin, Norfloxacin, etc.).
The Underestimated Danger - Embedded Bladder Infection:
From my experience working with various advisory groups, I know of many women whose bladder infections keep recurring despite all possible attempts at treatment,
or whose bladder remains permanently inflamed, even when a urine culture cannot detect any bacteria.
The bladder infection has, in a sense, become chronic.
The likely cause: The bacteria hide in the deeper layers of the bladder lining and in biofilms, where they are
resistant to antibiotics.
And how does this happen? The longer the germs remain untreated or unsuccessfully treated in the bladder,
the better they can establish themselves and eventually embed.
The resulting vicious cycle: With the renewal of the bladder lining, the "dormant" bacteria return to the bladder,
triggering an infection again, where they multiply
unchecked without treatment. Some of the new bacterial load re-embed in the lining. The cycle begins again.
Why am I telling you this? Because a targeted treatment with the appropriate antibiotic
(i.e., exactly what is sensitive to your specific bacteria, as indicated by a urine culture & antibiotic susceptibility test)
before they can embed and then torment you with painful infections for months or even years.
isn't a bad idea and ensures that the uropathogenic bacteria are "nipped in the bud"
before they become entrenched.
Such cases are often quickly considered "untreatable" in DACH, and some desperate women even agree to have their bladder removed.
A urological private clinic in London (Professor Malone-Lee †)
fortunately has a treatment plan for such cases.
More on embedded bladder infections and the London treatment protocol
under Is a bladder infection always detectable in urine?
Here is an overview of the pros and cons:
| Herbal Therapy (+ Painkillers) | Antibiotic |
|---|---|
| slow symptom relief | faster symptom relief |
| slightly increased risk of kidney infection | rare kidney infection |
| chronicisation (embedding) possible | chronicisation (embedding) rare |
| no damage to the microbiome | possible damage to the microbiome |
| few side effects | sometimes severe side effects |
| no resistance formation | possible resistance formation |
To start off with the topic of antibiotics, I recommend reading this in advance:
What are the pros and cons of antibiotic treatment?
Given the facts that up to two-thirds of uncomplicated urinary tract infections can heal spontaneously without antibiotics and the global development of resistance to antibiotics by bacteria can become a fundamental problem, it is recommended to try non-antibiotic treatments first for an uncomplicated urinary tract infection.
BUT - There is a kind of checklist that will make the decision "Antibiotic - Yes or No?" easier for you. The more of the following questions you can answer with YES, the more important it may be for you to use antibiotics:
- Are you in a risk group (child, man, pregnant woman)?
- Are you in menopause?
- Do you suffer from recurrent urinary tract infections (more than 3 UTIs per year or more than 2 UTIs in half a year)?
- Do you have comorbidities such as functional or anatomical urinary tract disorders, diabetes, kidney dysfunction, or immune deficiency?
- Do you have symptoms suggesting kidney involvement? For example, flank pain, painful kidney area, fever >38°C, chills, nausea, or vomiting.
- Have your symptoms not improved after 3-5 days?
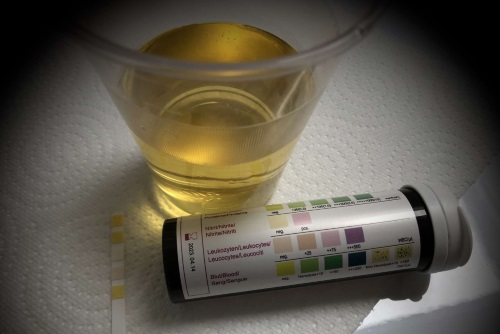
- Do the test strips on a urine test strip show elevated values for leukocytes and/or nitrite and/or blood?
- Is a bladder or urinary tract examination planned (this is generally not done during an acute infection)?
Participatory decision-making: The best treatment option should always be discussed and decided together with your doctor.
My tip - or rather - my command 🙂 to you:
On the internet, you often find that it can take several weeks for a urinary tract infection to heal on its own. If my symptoms and the urine test strip during self-treatment without antibiotics have not noticeably improved after 3-5 days, I have found that antibiotics have ultimately been necessary - even though I "fiddled around" for several weeks.
The command is therefore - and yes, I also have to pull myself together: 🙄
If you suspect a urinary tract infection, go to the practice, have your urine (preferably morning urine) tested and insist that the urine sample is sent for a urine culture with antibiogram
to a laboratory.
Are your symptoms severe and you don't know if you can hold on until the culture results?
Then ask your doctor to give you an emergency antibiotic (this falls under "calculated therapy" - it’s an antibiotic that, for example, has worked for you before in a UTI, or generally
has a broad spectrum of action and is recommended for UTIs according to guidelines). Only take the emergency antibiotic if you truly cannot wait for the antibiotic results from the antibiogram.
(Note: The antibiogram usually takes 2 - 4 days because the bacteria must be cultured on a growth medium and then tested for resistance against a range of antibiotics per grown bacterium).
Ideally, you would take an antibiotic according to the antibiogram that is sensitive to your bacteria even for an uncomplicated urinary tract infection, if necessary. If there are several options, choose the one that is best tolerated (no contraindications such as allergies, comorbidities, etc.) and has the fewest side effects & collateral damage (An example: the broader the spectrum, the more types of bacteria are destroyed, even where you need the bacteria, such as in the gut).
A summary table of recommended antibiotics for uncomplicated cystitis (including assessment of side effects, collateral damage, etc.) can be found here: S3 Guideline: Uncomplicated Urinary Tract Infections
You are probably asking yourself - Why should I go to all this trouble?
If you recover in a few days with natural remedies, wonderful!
You don't need to take any antibiotics.
But if the infection does not improve or even gets worse, at least you will have an antibiotic available that is sensitive to your bacteria
- even on weekends or public holidays.
In case of emergency, this process will save you a lot of suffering and protect you from a chronic urinary tract infection.
There are a number of antibiotics used for urinary tract infections. The medical S3 guidelines also provide clear recommendations on this.
Bladder infections (and subsequently kidney infections) are caused by various pathogens. Therefore, first and foremost: Not every antibiotic works for every pathogen. This is also why you should always urge your treating doctor to carry out a urine culture + antibiogram to determine the pathogen and the effective antibiotics when you present with symptoms of a bladder infection.
You might be wondering: If knowing the pathogen is so essential for treatment, why on earth doesn’t the medical staff encourage this right from the start? => Because the guidelines do not recommend it and because it is costly. Instead, a so-called "calculated therapy" with a "best guess antibiotic" is initiated.
The "best guess antibiotic" is usually chosen based on these criteria:
- Risk: Which patient group do you belong to? Are you pregnant? Do you already have symptoms of kidney involvement?
- Sensitivity: Which antibiotics are already resistant in your region?
- Pathogen spectrum: Against which (suspected) pathogens should the antibiotic work?
- Effectiveness: What percentage of pathogens are destroyed by a standard dose of the substance?
- Side effects: What unwanted side effects might occur due to your medical history (known allergies, kidney dysfunction, liver disease, etc.)
- Resistance situation: Is there a risk of collateral damage (resistances in you or the population)?
- Antibiotic Stewardship: Rational and responsible use of antibiotics => no reserve antibiotic should be used for an uncomplicated infection
By adhering to the above criteria, the following antibiotic groups should not be used for a purely "calculated therapy":
- Fluoroquinolones (all antibiotics ending in -floxacin): Serious side effects possible, collateral damage through the formation of multi-resistant pathogens
- Cephalosporins (all antibiotics starting with Cef-/Ceph-): Collateral damage through the formation of multi-resistant pathogens
- Fosfomycin (e.g. Monuril®): Intravenous use is considered a reserve antibiotic , therefore oral intake is not the first choice (even though it is an effective antibiotic and the guidelines classify it as preferred)
- Trimethoprim (e.g. InfectoTrimet®), Trimethoprim + Sulfamethoxazole (Cotrimoxazole): If the regional resistance situation for Escherichia coli is > 20 percent
So what remains, if the pathogen is unknown and you’re looking for an antibiotic to treat uncomplicated cystitis that works as effectively as possible - with few side effects and minimal collateral damage?
- Nitrofurantoin: Furadantin®, Nifuretten®, Nifurantin®, Uro-Tablinen® => very broad spectrum with exceptions: Proteus mirabilis and Pseudomonas aeruginosa are naturally resistant to Nitro (!)
- Nitroxoline: Nitroxoline forte, Nilox®
- Pivmecillinam: X-Systo® (Germany), Selexid® (Austria) => may also be used during pregnancy and breastfeeding
- Trimethoprim / Cotrimoxazole: InfectoTrimet® / Cotrim, Bactrim®, Eusaprim®, Kepinol® => In certain regions, however, unfortunately many pathogens are already resistant to this antibiotic
My experiences: Despite all these recommendations for antibiotic administration, far too many sufferers still go home after their doctor's visit with the following:
- Without a urine culture (no pathogen determination and no sensitivity analysis for antibiotics)
- Fluoroquinolone antibiotic or a single dose of Fosfomycin
My truly sincere tip:
- Be persistent! Don’t let them fob you off, demand a urine culture with an antibiogram!
- No -floxacin antibiotics! Accept a fluoroquinolone antibiotic only if there is no other choice (according to the antibiogram).
- Single dose with emergency dose: Ask for a second single dose if the symptoms are not noticeably reduced three days after taking the first dose
Here is an overview table for the recommended empirical short-term antibiotic therapy for uncomplicated cystitis in women of premenopausal age: S3 Guidelines: Uncomplicated Urinary Tract Infections
What to Do if You Have a Urinary Tract Infection (UTI)
When you have a urinary tract infection (UTI), it's essential to take the right antibiotics to ensure that the infection is fully cleared and doesn't recur. Here are some tips on what to do if you suspect you have a UTI:
Don't Take Any Antibiotics You Have at Home
- Only take antibiotics that your doctor has prescribed for you.
- A urine sample can only be taken after the last antibiotic intake, which is usually 3-5 days. Wait until then before visiting your doctor's surgery to provide a urine sample.
Tell Your Doctor You Want a Urine Test and Antibiotic Sensitivity Report
- When you visit your doctor, ask them to take a urine sample from you. This will help determine which antibiotics are most effective against the bacteria causing your UTI.
- Tell your doctor that you want an antibiotic sensitivity report (antibiogram). This is essential in finding out which antibiotics work best for your specific infection.
Ask Your Doctor About a Backup Antibiotic for Emergencies
- In case of an emergency, ask your doctor to prescribe a standard UTI antibiotic that you can take at home. Ensure this is not a fluoroquinolone.
- Request a second pack if the prescribed antibiotic is a single-dose one (like Fosfomycin). This can be helpful in cases where one dose may not be enough to clear the infection completely.
Follow Your Doctor's Instructions
- If you're prescribed an antibiotic, make sure you complete the full course as directed by your doctor. Don't stop taking it unless advised to do so by a medical professional.
- If you experience symptoms despite completing the antibiotic course, consider consulting another doctor or specialist who can help identify why the infection persists.
No! And that's for many reasons:
- Spectrum of action: Not every antibiotic works against every germ. Some antibiotics are naturally resistant, i.e., they cannot affect the bacterial strain by nature. For example, Proteus mirabilis and Pseudomonas aeruginosa are naturally resistant to nitrofurantoin.
- Individual risk: Existing allergies, intolerances, interactions with medications or contraindications (e.g. during pregnancy).
- Sensitivity: How many percent of the germs in the bacterial strain are sensitive to the antibiotic, how many are already resistant?
- Eradication rate: How many percent of the germs are killed by a standard dose of the antibiotic - i.e., how effective is the substance?
- Collateral damage: What is the risk of developing multi-resistant bacteria or Clostridium difficile-associated colitis?
- Antibiotic stewardship: Rational and responsible use of antibiotics => for a uncomplicated infection, no reserve antibiotic should be used!
You might also want to read the answers to:
What is the best antibiotic for cystitis?
Which antibiotics are taken for acute cystitis?
If you're still interested in Basics, Do's & Don'ts when selecting antibiotics, I can recommend the presentation "The 1x1 of ANTIBIOTIC THERAPY" from the LKH Universitätsklinikum Graz.
All substances that fight bacteria are considered antibiotics (AB) or antibacterial chemotherapeutics. Antibiotics were originally synthesised by microorganisms, such as penicillins, cephalosporins, aminoglycosides. Antibacterial chemotherapeutics are synthetically produced by humans, e.g. sulfonamides, metronidazole, quinolones. In a broader sense, however, antibiotics (AB) are the common term.
There are now 160 active ingredients (often chemically modified and no longer derived from natural substances like fungi) that have an antibiotic effect.
Antibiotics always work only on the pathogens of the disease, not on the inflammation (disease) itself. However, the inflammation heals because there are no pathogens left to trigger inflammatory reactions in the tissue.
Depending on their antibacterial effectiveness, an antibiotic can be classified into one of two groups:
- Bactericidal: These antibiotics inhibit growth and kill bacteria (penicillins, cephalosporins, carbapenems, fluoroquinolones, aminoglycosides, glycopeptides, metronidazole, fosfomycin).
- Bacteriostatic: These antibiotics inhibit bacterial reproduction. Dormant bacteria cannot be killed by them (macrolides, tetracyclines like doxycycline, clindamycin, linezolid, nitrofurantoin).
Antibiotics can also be classified by their mechanism of action:
- Inhibition of cell wall synthesis: Beta-lactam antibiotics (penicillins, cephalosporins, monobactams, carbapenems), glycopeptide antibiotics (vancomycin, teicoplanin, telavancin, dalbavancin), fosfomycin
- Nucleic acid metabolism (interference with bacterial DNA or RNA): Fluoroquinolones/quinolones (norfloxacin: reaches sufficient levels only in the urine, ofloxacin, ciprofloxacin, levofloxacin, moxifloxacin), nitroimidazole derivatives (metronidazole, nitrofurantoin), rifampicin
- Inhibition of bacterial protein synthesis: Macrolides (roxithromycin, clarithromycin, azithromycin), tetracyclines (doxycycline), aminoglycosides (gentamicin, amikacin), etc.
- Interference with tetrahydrofolic acid synthesis: Sulfonamides, trimethoprim => combined as cotrimoxazole (sulfamethoxazole + trimethoprim)
In addition to the antibacterial activity, the spectrum of activity of the substance is crucial:
- Narrow-spectrum antibiotics: These antibiotics target only a few gram-positive or gram-negative pathogens.
-
Broad-spectrum antibiotics:
These antibiotics target multiple pathogens with their mechanism of action, covering a "broad spectrum" of bacteria.
These include:
- Aminopenicillins
- Cephalosporins
- Fluoroquinolones
- Carbapenems
If you'd like to know more details about the individual substances, I recommend the following page: "Antibiotics Overview" by AMBOSS
The Problem with Resistances
Bacteria manage to outsmart antibiotics and ensure their survival through several mechanisms (e.g. they produce enzymes that render antibiotics ineffective or alter metabolic pathways that antibiotics would otherwise block, etc.).
Thanks to these mechanisms, entire bacterial strains become resistant to antibiotics. This happens more easily the more frequently bacteria come into contact with antibiotics (so the risk increases with each use). Bacteria can even transfer their resistance mechanisms from one bacterial species to another, resulting in the emergence of multiresistant strains that are resistant to multiple antibiotics at once.
Not every antibiotic fights all bacteria equally well. Some substances only kill a few types of bacteria (narrow-spectrum antibiotics), while others work against a wide range of bacteria simultaneously (broad-spectrum antibiotics or broad-spectrum antibiotics). Whenever possible, narrow-spectrum antibiotics should be used, as this leads to fewer resistances and fewer side effects. However, the bacteria (or bacteria) must first be identified through a bacterial culture. Only then can the "best antibiotic" be selected after the identified bacteria have undergone resistance testing (antibiogram).
In the case of severe infections or when there is a risk of an unfavourable course of the illness, it may still be reasonable to start treatment immediately with a broad-spectrum antibiotic after requesting a bacterial culture, as experience shows it is effective => empirical/calculated therapy. Once the result of the antibiogram is available after a few days, a switch to a suitable narrow-spectrum antibiotic can then be made.
The S3 guidelines provide clear recommendations on the selection, dosage, and duration of therapy.
Following the guidelines, the calculated/empirical short-term therapy should be preferred, especially for women in the premenopausal phase.
The short-term therapy (3 to 5 days) is preferred over the conventional therapy (7 to 10 days) for the following reasons:
- Better patient adherence (= adherence to the therapy)
- Fewer side effects (side effects = unwanted drug effects)
- Less resistance development: Lower selective pressure for resistant pathogens from the periurethral, vaginal, and fecal flora
As long as necessary, as short as possible!
For many years, it was believed that longer antibiotic therapies reduced the likelihood of infection recurrence or the development of resistance.
The still widely held belief: "Finish the pack". However, it is now known that such a simple rule is not sufficient for modern antibiotic therapy.
Today we know: the longer bacteria are exposed to the selective pressure of an antibiotic, the more likely it is that mainly resistant, i.e., antibiotic-insensitive pathogens, will survive.
Increasingly, studies show that for various infections, shorter antibiotic therapies are equivalent or even superior to longer therapies. A shorter antibiotic therapy not only has the advantage of fewer resistance developments but also leads to fewer side effects.
Another point we should be aware of: Underdosing leads to therapy failure . The dosage recommendations in the package insert usually follow a standard formula. For example, a woman weighing 56 kg and measuring 1.50 m is recommended the same dose as a man who is 1.90 m tall and weighs 90 kg.
In the future, the rule for antibiotics should be:
"The treatment should be as short as possible, but as long as necessary."
However, implementing this new credo is unfortunately not so straightforward:
- How long is "as long as necessary"?
- And what dosage is "as much as necessary"?
This depends on many factors, and there is no one-size-fits-all solution.
Duration of Therapy
The length of time an antibiotic needs to be taken depends on several factors, including:
- Type of the disease
- Severity of the disease
- Individual progression of the disease
- Triggering bacterial type
- Active substance of the antibiotic (for example, Nitrofurantoin 5-7 days, Trimethoprim 5-7 days)
Dosage
According to the recommendations of EUCAST (European Committee on Antimicrobial Susceptibility Testing), there are sufficient guidelines for adult dosage in clinical practice (both standard and high daily dosage).
The dosage of an antibiotic depends on several other factors, such as:
- Body weight: unusually high or low body weight
- Body composition: ratio of fat to muscle mass - adipose tissue influences the effect of a drug
- Organ health: breakdown of active substances by the liver and kidneys
The Big Danger: Under-dosing over a prolonged period
Most pathogens become resistant to antibiotics because the dosing is not high enough to eliminate as many/all germs as possible in the first step.
Some antibiotics develop resistance very quickly - aminopenicillins, cephalosporins, and macrolides. Low drug levels over a prolonged period likely play a major role in the development of resistance.
For example, the active ingredient of the macrolide antibiotic Azithromycin is measurable in plasma for a long time after the therapy ends. The consequence: In half of the patients who had received Azithromycin, scientists found erythromycin-resistant Streptococcus pneumoniae.
Conclusion: A few basics
I am convinced that it is really challenging to choose the best possible antibiotic therapy. It requires:
- Individual approach
- Comprehensive knowledge of optimal therapy for various conditions
- More precise monitoring of the respective disease progression
So basically, a medical expert with plenty of time for patients.
And although I am neither a doctor nor an expert, I would like to share with you a few thoughts that I "wrote behind my ears" after my thorough research.
- First, take a urine culture + antibiogram, then the antibiotic!
- Tips for the urine sample for the urine culture: First morning urine, the last bladder emptying should be more than 4 hours ago, before any antibiotic intake, immediately sent to the laboratory (or stored at 2-8°C)
- Targeted therapy is always better! A diagnostic test using urine culture and antibiogram clears many questions at once: Which antibiotics are sensitive?
- Calculated/Empirical therapy: Fosfomycin-trometamol, nitrofurantoin, and pivmecillinam have low resistance rates. Trimethoprim and cotrimoxazole have high resistance rates. No -floxacin antibiotics (fluoroquinolones)! More on this under Which is the best antibiotic for bladder infections?
- Dosing: sufficiently high (especially in cases of overweight). Kidney function should be monitored: Risk of under-dosing when adjusting the dose due to kidney insufficiency. Here you will find a reference table with standard dosing and high dosing: Resistance testing and antibiotic dosing
- Duration of therapy: a difficult topic... too long promotes resistance, too short may not eliminate all pathogens and promotes, for example, recurrent bladder infections.
- Therapy frequency: The pathogen sensitivity decreases as antibiotic use increases. This means the more frequently you take an antibiotic, the higher the risk of developing (multi)resistant pathogens.
A mixed infection refers to an infection with two or more organisms occurring simultaneously.
In a routine antibiogram**, a sensitivity test is usually performed for all the organisms found in the urine culture. You can find an example of a bacteriological report from a mixed infection with two organisms at this link.
The antibiotics that are effective against all the organisms involved in the infection should be used. This is known as a polymicrobial infection**. The choice of antibiotic will depend on the organisms present and their sensitivity patterns. Your healthcare professional will advise on the best course of treatment.
It's worth noting that Enterococcus faecalis, also known as Enterococcus faecium, are often found in mixed infections. However, whether these bacteria are pathogenic or not is still unclear. You can find more information about this at this link.
To prevent contamination, the urine sample should be handled correctly. You can find more information about this at this link. A further option to ensure that the sample is not contaminated during collection is to use a catheter to collect urine directly from the bladder.
Quick processing of the sample is also essential. It should be sent to the laboratory or stored at 2-8°C** as soon as possible. Bacteria can multiply quickly at room temperature and therefore contaminate the sample, affecting the test results. An example showing how quickly the bacterial count can increase over time can be found at this link.
Why is a Urine Culture done?
A Urine Test Strip (a rapid test) is a good way to determine if a urinary tract infection (UTI) is likely. Elevated leukocytes and/or erythrocytes indicate inflammation, nitrite suggests a nitrite-producing bacterial infection (E. coli, Klebsiella, Proteus Mirabilis).
If there is suspicion of a UTI, it is always beneficial to determine the causative organism (bacteria, fungus) - and that's exactly what a urine culture in a laboratory does.
If bacteria are found in the urine culture, the sensitivity/resistance against antibiotics is usually also determined - a so-called Antibiogram. The result of the Antibiogram shows which antibiotics can be used against the bacteria found in the urine culture.
The ideal sequence from symptom onset to antibiotic administration:
- Urine Test Strip => Suspicion of UTI
- Urine Culture => Determine causative organism and sensitivity/resistance against antibiotics
- Antibiotics => Administered based on Antibiogram results
The bacterial count is measured in CFU (colony-forming units). A colony on the plate (=culture medium) represents one CFU in the urine. It is counted exactly, and from a count of 100, it is estimated or compared to exact reference images. The count is always rounded up to the nearest ten. Depending on the volume of urine placed on the plate, the count is then multiplied by CFU/ml.
Generally, a bacterial count of 10^5 CFU/ml (100,000 CFU/ml) or more is considered significant and indicates a urinary tract infection. However, in the following cases, a bacterial count of less than 10^3 (1,000 CFU/ml) may also be an unambiguous sign of a clinically significant UTI:
- Clear symptoms of a UTI and/or leukocytes or nitrite in the urine
- Presence of antibacterial substances (positive inhibition test) in the urine
- In bacteria that generally do not multiply well in the urine, such as Staphylococcus saprophyticus
- At a short duration of urine retention (sample collection too quickly after bladder emptying)
- In cases of increased urination (excessive fluid intake, diuretic use, abnormal increased urination)
- With nephritis or kidney abscess
- In children's urine
- With biofilm formation => most bacterial cells are attached (growing on the surface) and only a few are planktonic in the urine
- In bacteria embedded in the bladder mucosa => only a few are planktonic in the urine
Firstly, it's essential to determine whether you have a complicated or uncomplicated UTI. Complicated UTIs are often associated with symptoms like fever, chills, or a severe burning sensation during urination. In these cases, antibiotics should not be delayed until the urine culture results are available.
Instead, a broad-spectrum antibiotic is usually prescribed immediately to cover possible pathogens and to start treating the infection promptly.
General Principles
- In uncomplicated UTIs (without fever or blood in urine), it's recommended to perform a urinalysis before starting antibiotics.
- Before prescribing an antibiotic, the clinician should consider the following factors: • The severity of symptoms • Past medical history, including allergies and sensitivity to specific antibiotics • Pregnancy status (if applicable) • Any relevant comorbidities or complications
General Antibiotics for UTI
The general choice of antibiotic should cover the most common pathogens, such as E. coli, Proteus mirabilis, and others.
What antibiotics are commonly used for UTI?Specific Antibiotics for UTI
For complicated UTIs or those with fever and blood in urine, more specific antibiotics may be chosen based on the urinalysis results.
What are some common antibiotics for uncomplicated and complicated UTI?General Antibiotics
The general choice of antibiotic should cover the most common pathogens, such as E. coli, Proteus mirabilis, and others.
What antibiotics are commonly used for UTI?An antibiogram is used in a microbiological laboratory to test which antibiotics are effective against the pathogen(s) found in the urine culture.
Why perform an Antibiogram?
The antibiogram is helpful because no antibiotic is effective against all possible pathogens. Not only because not every antibiotic works against every pathogen (natural resistance), but also and especially in times of increasing multi-resistance, it is more important than ever to handle antibiotic therapy carefully.
Unfortunately, the current practice is often as follows: One antibiotic after another is prescribed until one is found that works. This uncritical use of antibiotics unnecessarily harms the microbiome and promotes resistant pathogens.
How is an Antibiogram performed?
The starting point for the antibiogram is a detected pathogen. In the case of bladder infections, the pathogen(s) are usually identified in a urine culture.
There are two different methods for performing the antibiogram:
- Agar diffusion test
- Dilution method
In the agar diffusion test, the pathogen to be tested is spread over a plate with a nutrient medium. The plate is then covered with circular discs containing various antibiotics in defined amounts. During incubation, the pathogens grow towards the disc until a concentration of the antibiotic is reached that is sufficient to inhibit growth, creating a so-called inhibition zone around the disc. Each antibiotic has outer and inner target inhibition zone sizes. If the measured inhibition zone is:
- outside the outer target value, the pathogen is sensitive (S)
- within the inner target value, the pathogen is resistant (R)
- between the outer and inner target limits, the pathogen is classified as intermediate (I)
The larger the inhibition zone, the more sensitive the pathogen is!
In the dilution method, a more precise approach is used to determine the Minimum Inhibitory Concentration (MIC) for various antibiotics against the identified pathogen.
The MIC is the smallest concentration of an antimicrobial substance (e.g. an antibiotic) that still prevents the pathogen from growing in the culture.
In the microdilution method, the pathogen is mixed with a defined amount of an antibiotic in a liquid nutrient medium in a microtiter plate.
A dilution series with different concentrations of the antibiotic is performed (1, 2, 4, 8, 16, 32 mg/L).
The growth of the microorganism is indicated by a cloudiness in the nutrient medium.
The mixture with the lowest concentration of the antibiotic where the liquid remains clear provides the MIC value.
The smaller the MIC, the more sensitive the pathogen is!
How is an Antibiogram interpreted?
Depending on the method, the result for each tested antimicrobial substance will either be Sensitive (S), Intermediate (I), and Resistant (R), or the Minimum Inhibitory Concentration (MIC) + interpretation of S-I-R.
S-I-R is interpreted as follows:
- S = Sensitive => high probability of therapeutic success with standard dosage
- I = Sensitive with dosage recommendation => high probability of therapeutic success with increased exposure through an adjusted dosage regimen or through concentration at the infection site
- R = Resistant => high probability of therapy failure
You can find the dosage tables for standard and high dosages at the National Antibiotic Sensitivity Testing Committee (NAK) under Resistance Testing and Antibiotic Dosage.
To illustrate, here is an example of an antibiogram for a mixed infection with two pathogens.

The standard dosage for Amoxicillin/Clavulanic acid for uncomplicated UTIs (excerpt from the NAK reference table): 3 x daily 0.5 g Amoxicillin + 0.125 g Clavulanic acid, oral.

The presence of three or more potentially uropathogenic bacterial strains is most likely due to contamination. In such cases, no resistance determinations are made and the submission of a sterile urine sample is recommended.
In particular, when mid-stream urine is collected, contaminating bacteria are often found due to incorrect collection. Urine is a (nearly) sterile bodily fluid. However, as the anterior urethra is physiologically colonised with bacteria, contamination can occur during urine collection. The most common contaminants include:
- coagulase-negative Staphylococci (except S. saprophyticus)
- greening Streptococci
- Enterococci: often after antibiotic therapy
- Coryneform bacteria
- Propionibacterium
- Lactobacillus sp.
- Candida (fungi): often after antibiotic therapy
To help you get into this topic, I recommend reading the article: How do you know which antibiotic works?
Trap #1: The bacteria are resistant => The antibiotic can't work at all
After reading the article, one key point will have stuck with you: An antibiotic treatment without knowing the causative pathogen always carries the risk of being unsuccessful.
- The pathogen may be naturally resistant to the antibiotic. For example, Mycoplasma bacteria have no cell wall and are therefore resistant to β-lactam antibiotics (all cell wall synthesis inhibitors, including Fosfomycin).
- The pathogen may have already developed a resistance to the antibiotic.
The solution: Urine culture + Antibiogram. In my view, it is essential that a culture is taken from your urine to identify the pathogen(s) before the first dose of antibiotics is administered. The antibiogram will clearly show which antibiotics are effective against your pathogen(s). You can view an example of such a result here: Example of a bacteriological report of a mixed infection with two pathogens.
Trap #2: Too low a dose and/or too short a therapy
The symptoms improve slightly, but the UTI doesn't heal completely. Too many pathogens remain (possibly now with more resistance mechanisms) and after a few days or weeks, the inflammation flares up again. Although short-term therapy (single dose or 3 days) is often preferred, I'm not particularly fond of it. Even less so am I a fan of insufficient dosages, as this promotes resistance - the pathogens have far too much room to develop resistance under the selective pressure.
Conclusion: It's better to shoot with a targeted cannon, and put the shotgun aside.
The very commonly prescribed classic in Trap #2: The antibiotic Fosfomycin as a single dose (Monuril®). Fosfomycin is a good active ingredient and, moreover, a reserve antibiotic, but a single dose is often insufficient to overcome the pathogen load. According to a study comparing it with Nitrofurantoin, nearly half of the participants were still not symptom-free 28 days after the end of therapy.
The solution: No single dose (or at least another single dose after three days), therapy duration at least 5 days, better a higher dose (if individual circumstances allow) than underdosing.
Trap #3: The pathogens are hiding
Bacteria unfortunately always find ways to protect themselves from an antibiotic attack. Especially with UTIs, there are two ways in which the pathogens hide:
- In the biofilm: Bacterial colonies are protected by a self-produced extracellular polymeric matrix, the biofilm.
- In the urothelium (embedded pathogens): Intracellular bacterial communities => Uropathogenic bacteria can also invade the urothelial cell and form a biofilm-like community there. This protects the bacteria from the immune system, is the trigger for recurring UTIs, and can cause symptoms even when standard diagnostics can't detect a UTI.
In the biofilm and urothelium, bacteria survive up to 1,500 times higher antibiotic concentrations.
Learn more on the topic at Is a UTI always detectable in urine?
The solution to this problem is unfortunately not simple, and there are various approaches, with differing levels of testing and reliability:
- Forskolin* to eliminate intracellular bacteria. Alternatively, Chitosan* acts as a bladder wall exfoliant (removing the superficial layer of bladder cells).
-
Biofilm inhibitors:
- Phytopharmaceuticals: For example, nasturtium and horseradish ( Angocin® Anti-Infekt N* ), arbutin (from bearberry leaves), coumarins.
- N-Acetyl L-Cysteine (NAC): Antioxidative, anti-inflammatory, and mucolytic (mucus-dissolving); destroys and reduces biofilm formation by bacteria and fungi.
- Lactoferrin: The enzyme lactoferrin deprives bacteria of essential nutrients like iron, preventing biofilm formation as bacteria continually search for nutrients. Lactoferrin is a natural peptide found in tears, saliva, and breast milk.
- Enzymes (e.g. nattokinase, serrapeptase): Interfase® Plus - Klaire Labs, Biofilm Defense® - Kirkman®
- Long-term antibiotic therapy in combination with the urinary tract disinfectant Hiprex® (e.g. in the private clinic at Harley Street 10 in London).
- Phage therapy: Phages are viruses that attack and dissolve bacteria (including in biofilms and dormant bacteria called persisters). Phage therapy is still practiced in countries of the former Eastern Bloc. Phages are host-specific, meaning they target a specific bacterial species.
Trap #4: It’s Something Else
If there are no typical uropathogenic bacteria colonizing you, then (standard) antibiotics can do little to help. Sometimes, rare pathogens (often sexually transmitted) require special detection methods (e.g. PCR, microscopy), such as:
- Infection with sexually transmitted bacteria: Gonococci, chlamydia, mycoplasma, ureaplasma, trichomonas (protozoa). They often cause symptoms in the urethra => urethritis (inflammation of the urethra).
- Infection with fungi: Usually candida species but also aspergillus => Detection through microscopic urine examination.
- Infection with parasites: Urogenital schistosomiasis (bilharziasis) => Microscopic detection of schistosomes.
- Infection with rare pathogens: Non-tuberculous mycobacteria, anaerobes (Peptococcus and Peptostreptococcus), Gardnerella vaginalis
- Infection with viruses: The herpes simplex virus can infect the urethra, cause pain during urination, and lead to problems emptying the bladder. . A BK (polyoma) virus infection can lead to cystitis with visible blood in the urine, particularly in immunosuppressed patients.
Not all cases of pain, burning, or frequent urination are caused by bacterial inflammation.
- Obstructions: Bladder stones, kidney stones, urethral diverticula, tumours (bladder cancer).
- Endometriosis: A painful condition where uterine lining tissue (endometrium) grows outside the uterus (e.g. on the ovary or bladder).
- Vaginitis: Vaginal inflammation can cause symptoms similar to cystitis.
- Vulvovaginitis: Inflammation of the female external genitalia, including the vagina.
- Vulvodynia / Vestibulodynia: Itching, burning, stinging, dryness, soreness, or pain in the external female genital area. Sometimes also affecting vaginal, pelvic floor, or anal areas.
- Salpingitis: Inflammation of the fallopian tube.
- Overactive bladder (OAB): Chronic irritation of the lower urinary tract, causing symptoms similar to a UTI (frequent and painful urination), but urine tests show no abnormalities. Symptoms are typically less severe at night.
- Radiation: Bladder inflammation following radiotherapy.
- Mechanical or chemical irritation: For example, due to bladder catheters, medications (painkillers, chemotherapy).
- Urinary retention issues: Mechanical bladder emptying obstruction (e.g. urinary tract blockages, urethral stricture), neurogenic bladder emptying issues (nerve damage in the brain or spinal cord).
- Pelvic organ prolapse (bladder prolapse): Impaired bladder function (incontinence, residual urine), increased susceptibility to bladder infections.
- Musculoskeletal and connective tissue disorders: Pelvic floor hypertonicity, lumbar spine disc problems, etc.
- Gastrointestinal disorders: Irritable bowel syndrome, leaky gut, etc.
- Interstitial cystitis / Bladder Pain Syndrome (IC/BPS): A non-infectious, chronic bladder condition with symptoms resembling bladder infections. The exact cause is unclear, making IC/BPS a diagnosis of exclusion. Due to damage in the bladder’s protective lining, irritating substances from urine penetrate deeper layers of the bladder wall, causing inflammation.
- Histaminosis (mast cell activation syndrome MCAS, histamine intolerance): Excess histamine due to overactive immune defense of mast cells in MCAS, or a metabolic disorder in histamine intolerance, can lead to chronic bladder inflammation.
The solution: Don’t give up and keep searching. Be sure to have everything thoroughly checked gynaecologically. Consider and rule out all differential diagnoses. I know of several cases where urologists unsuccessfully treated chronic bladder infections for years, only for a gynaecologist to discover the root cause was endometriosis.
Conclusion: Use antibiotics carefully & think outside the box
What certainly doesn’t help (apart from creating more resistant bacteria):
Trying one antibiotic after another in the hope that the nth one will work.
Even the perfectly matched antibiotic can only successfully combat the bacteria if it is used correctly.
Consistent active ingredient levels are crucial
It is important to take the medication as prescribed, because only then will there be a sufficiently high concentration of the active ingredient in the body to eliminate the pathogens. If the antibiotic cannot fully develop its effect (e.g. due to inaccurate intake or premature discontinuation), the therapy may fail. And the much worse consequence: resistant bacteria may survive and become resistant to the antibiotic.
-
Correct timing: Three times daily does not mean upon waking, at lunch, and at dinner.
- 1x daily: Take the tablet (prescribed dose) approximately every 24 hours, e.g. always in the morning at the same time.
- 2x daily: Take the tablet about 12 hours apart, e.g. one at 8:00 a.m. and one at 8:00 p.m.
- 3x daily: Take the tablet about every 8 hours, e.g. the first dose at 7:00 a.m., the second dose after lunch at 3:00 p.m., the third dose before bedtime at the earliest 10:00 p.m.
- Correct dosage: Caution! Some antibiotics (e.g. doxycycline) are given at higher doses at the start of treatment to quickly reach the required active ingredient concentrations.
- Do NOT take with milk, tea, coffee, antacids, mineral supplements (calcium, magnesium, or zinc): Taking these at the same time as antibiotics can hinder the absorption of the active ingredient in the stomach.
- Plenty of water: Take with a large glass of water - not just a sip! Otherwise, there is a risk of the medication getting stuck in the oesophagus, which can even damage the tissue.
- Not lying down immediately: Tablets can adhere to the oesophagus when lying down and damage the tissue there. Always follow the package insert instructions, e.g. do not lie down for 1–2 hours after taking doxycycline.
-
Follow package insert instructions: Manufacturers provide detailed instructions in the package leaflet, which should be strictly followed, such as:
- Before meals: Take the tablet half an hour to one hour beforehand (reason: Some active ingredients are less well absorbed if taken with food).
- With meals: Take the tablet directly with a meal.
- Interaction check: Some antibiotics have potentially dangerous interactions with other medications, e.g. macrolide antibiotics (erythromycin, etc.) and cholesterol-lowering drugs (statins) - the statin's effect is enhanced. Other examples: blood sugar fluctuations in people with diabetes, increased bleeding tendency, etc. A practical service from Apotheken Umschau is the Interaction Check, where you can easily check if your medications have interactions.
-
Adherence to therapy:
- Don’t forget: Set reminders in your smartphone calendar or use dedicated apps. Should you skip or make up for missed medication? This depends on the active ingredient.
- Don’t stop prematurely: Even if symptoms improve, treatment should never be stopped without consulting a doctor.
- Fear of side effects: The package leaflet must list all known side effects; however, not every patient will experience them. Learn how to interpret side effects from the leaflet in an article from Apotheken Umschau: Side Effects: What You Should Know.
Stopping antibiotics prematurely can lead to the worsening of the infection. When symptoms subside, the bacterial cultures may only have been reduced, leaving enough pathogens in the body for a relapse. This can result in a recurrence, particularly in cases of a weakened immune system.
However: The course of the illness and the severity of a UTI are very individual. While some experience symptom relief the day after starting treatment, others may endure symptoms for several days.
Basic rule: Follow the prescription
The basic rule for taking antibiotics is to follow the prescription:
- Take them for the prescribed duration, even if symptoms improve.
- Do not take less than the recommended dose.
- Follow instructions for use: What should I keep in mind when taking antibiotics?
- No improvement? => Contact your doctor.
-
Experiencing side effects? => Consult your doctor before stopping the medication. Typical side effects include:
- Itching
- Rash
- Swelling
- Muscle and tendon pain
My advice: If you feel the antibiotic is not working, or if symptoms persist towards the end of the treatment (e.g. after a single dose of fosfomycin or a 3-day course), contact your doctor immediately. You may need a different antibiotic or an extended treatment duration.
Not every side effect is a true allergy
An estimated four out of five reactions to a medication are not allergic but rather "normal" side effects. Never stop taking medication on your own, even if you feel it’s not effective or if there are too many side effects - always consult a doctor. They can determine if it's truly an allergy and, if necessary, provide an alternative medication.
Caution: Some people do have true allergic reactions to certain antibiotics. Allergies to antibiotics like penicillin are the most well-known. Severe allergic reactions can, in rare cases, cause life-threatening breathing or cardiovascular problems. If you suspect an allergy, seek medical attention immediately. In most cases, alternative drug classes are available.
Stopping early does not necessarily lead to resistance
As with any other medication, the rule for taking antibiotics is: as short as possible, but as long as necessary.
The widespread assumption that stopping antibiotics too early generally creates more resistant bacteria (compared to completing the entire course) is, according to studies from England, scientifically unproven. (Note: Certain bacterial strains and medications may be exceptions, e.g. with tuberculosis, pathogens can develop resistance due to stopping therapy early).
The majority of resistance develops through so-called "collateral selection". Everyday bacteria, which usually do not cause illnesses, develop resistance through long-term antibiotic treatment and can thus become a threat to the affected person.
Selection, dosage, and duration of therapy
The S3 Guideline provides clear recommendations regarding selection, dosage, and duration of therapy: Which antibiotics are used for acute bladder infections?
For premenopausal women, empirical short-term therapy (3-5 days) is recommended. Ultimately, the treating doctor decides on the optimal duration of intake, tailored specifically to the infection and the expected course.
In this FAQ, you can read about the advantages and disadvantages of shorter or longer antibiotic treatments: What is better? A short-term therapy (3-5 days) or a standard therapy (5-10 days) with antibiotics?
In Germany, Austria, and Switzerland, antibiotics are subject to a prescription requirement (also known as a prescription-only medication). This means in practice that antibiotics are not available over-the-counter and a prescription is always required.
Some online services for getting antibiotics are much more expensive than the classic visit to the doctor/GP. Online portals also do not take a urine culture, so they can only initiate a calculated therapy with antibiotics based on a questionnaire. For me, this means that I am not convinced of the necessity 100%. It is probably always better to find a GP who initiates treatment...
Nitrofuran derivative Furazidin
The antibacterial Furazidin is available over-the-counter in Poland and has a similar mechanism of action to Nitrofurantoin. It acts against both gram-positive (Staphylococcus epidermidis, Staphylococcus aureus, Staphylococcus faecalis) and gram-negative microorganisms (Enterobacteriaceae – Salmonella, Shygella, Proteus, Klebsiella, Escherichia, Enterobacter etc.). It is used to treat urinary tract infections.
My conclusion
Online services for getting antibiotics are much more expensive than the classic visit to the doctor/GP. Also, online portals do not take a urine culture and can only initiate a calculated therapy with antibiotics based on a questionnaire. For me, this means that I am not convinced of the necessity 100%.
Antibiotics Natural antibioticsAll antibiotics have side effects, and any antibiotic can rarely cause severe side effects.
The key difference in this context is: how often do severe side effects occur, and are they reversible?
Floxed!
A group of antibiotics unfortunately still popular for urinary tract infections is the fluoroquinolones. This includes substances ending with -floxacin, such as ciprofloxacin, levofloxacin, moxifloxacin, norfloxacin, and ofloxacin. Despite this, a Red Hand Letter was issued in 2019 regarding the use of fluoroquinolone antibiotics.
The reason: Severe and persistent side effects that impact quality of life and may be irreversible, mainly affecting the musculoskeletal system and nervous system.
Recommendations:
- Not for uncomplicated cystitis
- Not for recurrent lower urinary tract infections
The only exception: If all other antibiotics usually recommended for these infections are deemed unsuitable. And even then, never in combination with corticosteroids.
What does this mean for you?
You should always refuse fluoroquinolone antibiotics unless there is no alternative, which is very rarely the case.
If you must take fluoroquinolone antibiotics, you should immediately stop the treatment at the first signs of these severe side effects:
Severe side effects affecting the musculoskeletal system include:
- Tendinitis (tendon inflammation) and tendon rupture
- Myalgia (muscle pain), muscle weakness
- Arthralgia (joint pain), joint swelling
- Gait disturbance
Severe side effects affecting the peripheral and central nervous system include:
- Peripheral neuropathy (various nerve damages): sensory disturbances, abnormal sensations such as tingling, burning, or "pins and needles", disturbances in touch, pain, or temperature sensitivity, etc.
- Insomnia
- Depression
- Fatigue
- Impaired memory
- Visual, auditory, olfactory, and taste disturbances
Conclusion
For a long time, I was also unaware of the issue. I consider myself lucky that the antibiotics like Cipro and others never caused severe side effects for me. Unfortunately, through support groups, I know of numerous cases where people suddenly can hardly walk or experience severe neurological impairments.
Yet many doctors routinely prescribe these medications for minor infections. It’s incomprehensible – because fluoroquinolones should really only be used for more serious infections, when no alternatives are available.
WARNING! The most common interactions with other medications
- Statins (=cholesterol-lowering drugs) and macrolides: The interaction between macrolides (roxithromycin, clarithromycin, azithromycin) and statins is classified as severe. There is a risk of myopathies (muscle disorders) and rhabdomyolysis (breakdown of muscle fibres). Macrolides are used for infections caused by pathogens such as chlamydia, mycoplasma, streptococci, and gonococci.
- Antiarrhythmics and fluoroquinolones: When fluoroquinolones are combined with other QT interval-prolonging drugs, such as antiarrhythmics of classes IA and III (medications for heart rhythm disorders), there is an increased risk of cardiac arrhythmias (ventricular arrhythmias, torsades de pointes). Fluoroquinolones (all antibiotics ending with -floxacin) are often unnecessarily prescribed for UTIs. Macrolides can also prolong the QT interval in the ECG, so caution is also required when macrolides and antiarrhythmics are taken together.
- NSAIDs (e.g. IBU) and fluoroquinolones: When non-steroidal anti-inflammatory drugs (NSAIDs) (except acetylsalicylic acid) are taken together with fluoroquinolones, significant, clinically relevant interactions occur => NSAIDs amplify the neurotoxic side effects of fluoroquinolones by up to 300 times. So: Do not take NSAIDs such as ibuprofen/diclofenac together with fluoroquinolones (all antibiotics ending with -floxacin)!
A great article on toxic effects: Toxic effects of selected antibiotics
Gastrointestinal issues
Antibiotics do not differentiate between harmful and beneficial bacteria; they affect all bacteria in the human body within their spectrum of activity. Thus, they destroy not only the culprits (e.g. E. coli in the urinary tract) but also the beneficial bacteria in the gut and vagina. The result is often a bacterial imbalance – a disrupted microbiome.
An antibiotic-induced gut flora disruption often manifests as diarrhoea, stomach pain, and nausea. In cases of bloody diarrhoea or severe abdominal pain, it could indicate a life-threatening inflammation of the colon (pseudomembranous colitis), caused by antibiotic-associated overgrowth of Clostridium difficile.
Countermeasure: Probiotics: For bloody, slimy, or cramping diarrhoea, return to your doctor immediately.
For mild diarrhoea, you can counteract with probiotic products even during antibiotic treatment.
Probiotics aim to repopulate the beneficial bacteria in the gut.
Often, the gut recovers on its own, but sometimes diarrhoea persists despite probiotics. In such cases, I recommend a stool analysis.
The results will provide targeted recommendations for replacing the missing bacterial strains.
Fungal infections
An antibiotic-induced vaginal flora disruption often leads to fungal infections, sometimes with a delay of 1-2 weeks. Due to the drastic reduction of protective lactobacilli caused by antibiotics, pathogenic yeasts, most commonly Candida albicans, proliferate. A vaginal yeast infection (vaginal mycosis) increases the risk of a subsequent urinary tract infection, thus perpetuating the vicious cycle.
Countermeasure: Lactic acid and lactobacilli: A yeast infection is unpleasant, and its treatment further affects the vaginal flora. If you are prone to yeast infections, the motto should be: Prevention is better than cure!
- Only use lukewarm water for cleansing down under
- Wear breathable cotton underwear and avoid panty liners
- Preventatively use local treatments with lactic acid and lactobacilli alternately
Do you suspect a fungal infection?
- Ideally, visit your gynaecologist for a swab test
- Alternatively, an antifungal medication (vaginal suppositories and creams) from the pharmacy containing one of the following active ingredients: Clotrimazole, Miconazole, Nystatin
- Do not use products for vaginal restoration with lactic acid during fungal treatment!
- Only after fungal treatment rebuild the vaginal flora with lactic acid and lactobacilli alternately
Allergic reactions
According to specialists, only about 2-3% of the population truly suffer from an antibiotic allergy.
In the worst case, an allergic individual might experience an anaphylactic shock approximately 30 minutes after ingestion – causing a circulatory collapse and necessitating immediate hospitalisation.
However, reactions such as skin rash, redness, and itching are usually "just" a hypersensitivity reaction – an individual, unpredictable response to the antibiotic.
In any case of such overreactions, you should consult your treating doctor.
Often, the simplest solution is to switch to a different, effective antibiotic.
Tendonitis, nerve damage, and psychosis
These side effects can occur with the use of fluoroquinolone antibiotics.
Learn more at Which antibiotics have serious side effects?
Overview table
Maybe!
Antibiotics and their active substances have no direct or immediate effect on the efficacy of contraceptive pills (except for the TB antibiotic Rifabutin). However, here's the thing: Antibiotics have a very common and for some contraceptive pills fatal side effect - stomach and intestinal discomfort, i.e. vomiting and diarrhoea.
Especially broad-spectrum antibiotics destroy a large part of the bacteria flora in the gut. This often leads to diarrhoea. Diarrhoea means that the active ingredients of the pill are only reducedly absorbed, and therefore the contraceptive effect may not be guaranteed.
If you need to vomit within 3 hours after taking the pill, you can take it again within the next 12 hours. If you vomit multiple times, the protection for that month is not guaranteed.
Conclusion: If you don't experience vomiting or diarrhoea from the antibiotic intake, there's nothing to worry about. However, if you're unable to go to the loo or need to vomit (even if you're not taking antibiotics!), then use an additional method of contraception, such as a condom or diaphragm for that monthly cycle.
Pregnancy and breastfeeding are particularly sensitive periods during which medication should ideally be avoided. However, medically necessary medications, such as antibiotics for a bacterial infection, are exceptions. Untreated infections can harm the mother and sometimes the child.
Urinary tract infections during pregnancy must be treated, as there is a risk of kidney infection (pyelonephritis gravidarum) and associated preterm birth.
Which antibiotics can be used during pregnancy is best determined by your gynaecologist.
Typically, the following antibiotics are suitable for cystitis or pyelonephritis:
- Penicillins: Ampicillin, Amoxicillin (unfortunately, often ineffective due to resistant pathogens)
- Pivmecillinam: Narrow-spectrum penicillin, Selexid®, Pivmelam®, X-Systo®
- Macrolides: Azithromycin, Erythromycin
- Cephalosporins: Cefalexin, Cefuroxime, Cefuroxime, Cefixime, Cefadroxil (except Cefpodoxime)
- Fosfomycin: Second-choice medication, as there is limited information about its use during pregnancy.
The following antibiotics, often used for urinary tract conditions, are contraindicated (=not suitable) during pregnancy:
- Fluoroquinolones: Ciprofloxacin, Ofloxacin, Moxifloxacin, Norfloxacin, Levofloxacin
- Trimethoprim and Trimethoprim-Sulfamethoxazole (due to its effects on folic acid balance)
- Nitrofurantoin and its derivatives (especially not during the last three months before birth)
- Tetracyclines, such as Doxycycline (e.g. for urethritis caused by sexually transmitted pathogens)
- Aminoglycosides
The degree of potential toxicity always depends on the developmental stage of the fetus.
More than 40% of pregnancies are unplanned
Considering that over 40% of pregnancies are unplanned, women of childbearing age (20% of the German population) should be regarded as a target group for patients requiring pregnancy-compatible medication.
This is particularly important during early pregnancy (embryonic phase: weeks 3 to 8, when internal and external organs are formed), as the risk of congenital severe malformations and permanent organ damage is highest.
Tip: embryotox.de
The Berlin Charité provides embryotox, an internet portal offering independent information on the safety of medications during pregnancy and breastfeeding. They also offer free, individual consultations.
Most medications are present in breast milk. How much reaches the infant’s system depends on several factors (active ingredient, amount of breast milk, etc.). Some medications, even in minute quantities, can harm the baby.
Young infants under two months (especially preterm infants) are more sensitive to the mother’s (long-term) medication than older infants.
A threshold of 10% of the therapeutic dose has been arbitrarily chosen as a limit for low and clinically insignificant exposure. The exposure index is calculated as the daily dose of the drug consumed by the child (the product of the time-averaged drug concentration in breast milk and the daily breast milk intake – approximately 150 ml/kg body weight) relative to the therapeutic dose.
With many antibiotics, the infant receives less than 1% of the body-weight-adjusted therapeutic dose – these levels are not considered clinically relevant.
Most breastfed infants show no symptoms. In isolated cases, “drug-laden” breast milk may cause looser stools, rarely diarrhoea.
Mothers should generally prefer medications that only need to be taken once a day. These should be taken before the infant’s longest sleep period or immediately after breastfeeding.
Similar to during pregnancy, Pivmecillinam, Penicillins, Cephalosporins, and Macrolides are preferred.
Furthermore, the following antibiotics are also possible during breastfeeding:
- Fosfomycin: After a single dose of Fosfomycin, breastfeeding can continue without interruption.
- Amoxicillin and Clavulanic acid: Depending on the pathogen spectrum, the combination of Amoxicillin and Clavulanic acid can be used during breastfeeding.
- Cotrimoxazole: If required by the pathogen spectrum, breastfeeding can also continue with Cotrimoxazole.
- Ciprofloxacin: If required by the pathogen spectrum, breastfeeding can also continue with Ciprofloxacin.
- Nitrofurantoin: If Nitrofurantoin therapy is absolutely necessary, breastfeeding can continue with this medication. Since only a small amount of Nitrofurantoin passes into breast milk, a bladder infection during breastfeeding should preferably be treated with other substances.
After pregnancy, it's often before pregnancy
Even while breastfeeding, a new pregnancy can occur during the reproductive years. Therefore, when starting a new medication during breastfeeding, pregnancy-compatible drugs should be preferred.
Beware of resistances
Although a wide range of antibiotics is classified as safe during breastfeeding, the discussion about the potential development of resistant pathogens in infants is not yet concluded.
Fact: A small amount of the medication passes into the breast milk and to the baby.
Unclear: To what extent this small amount contributes to the development of resistance.
Tip: embryotox.de
The Charité in Berlin provides embryotox independent information on the safety of medications during pregnancy and breastfeeding on their website. They also offer free individual consultations.
One thing upfront: Before starting antibiotic therapy, a urine culture must always be taken in children to identify the pathogen and determine appropriate antibiotics (=> antibiogram).
If an antibiotic is needed before receiving the antibiogram (=> calculated/empiric therapy), the selection depends on the local resistance situation and the child's age. After receiving the antibiogram (which can take a few days), treatment is tailored according to the age and antibiogram-guided monotherapy.
The dosing is age- and weight-dependent.
Very ill children and newborns receive antibiotics via intramuscular injection or intravenously. Other children take antibiotics orally. The treatment usually lasts 7 to 10 days.
First-line antibiotics according to guidelines:
- Trimethoprim (with or without Sulfamethoxazole) for E. coli resistance rates below 20% (Infectotrimet®, Lidaprim®, Bactrim®, Cotrim®)
- Amoxicillin/Clavulanic acid (e.g. Xiclav®, Amoxiclav®, Clavamox®, Augmentin®)
- Nitrofurantoin (after the 3rd month of life, e.g. Furadantin®, Nifurantin®)
- from 6 years: Pivmecillinam (e.g. Selexid®, X-Systo®)
- from 12 years: Fosfomycin (e.g. Monuril®)
- from 14 years: Nitroxolin
According to guidelines, highly effective reserve antibiotics (e.g. Ciprofloxacin and 2nd or 3rd generation Cephalosporins - Ceftriaxone, Cefotaxime or Ceftazidime) should generally not be used to treat uncomplicated cystitis in children and adolescents. And although Cefaclor seems particularly suitable, it should not be prescribed for uncomplicated cystitis in children and adolescents, if possible.
The reason for this: Resistance development with Cephalosporins. The impact of Cephalosporins on the selection of ESBL (Extended Spectrum Beta-Lactamase) producing bacteria, which are increasingly found in paediatric urinary tract infections according to the guidelines, is particularly problematic. Cephalosporins are highly effective antibiotics whose potency must also be preserved for infections in other organ systems.
Nevertheless, unfortunately, Cephalosporins have now become standard therapeutics when children are infected with the urinary tract and bladder – possibly involving the kidneys. This is particularly true for regions where there is already a high resistance rate against Trimethoprim, the former standard medication for urinary tract infections.
The sad truth in the end: A 2016 study by BKK unfortunately found that antibiotics are prescribed much more frequently to children than to adults. Furthermore, it is rare that microbiological confirmation through antibiogram is conducted.
Therefore, my appeal to you: Please advocate for your child. Encourage the doctor to send a urine sample to determine which uropathogenic germ (or germs) is causing your child’s issue. This will also clarify which antibiotics will be effective, and it won’t be necessary to indiscriminately use broad-spectrum antibiotics.
If the urinary tract infections keep recurring, essentially "chronic", you can try long-term prophylaxis with antibiotics. By long-term prophylaxis, several things can be meant, e.g. regular intake of AB after intercourse or a daily sustained intake of a reduced dose of AB over a period of 3-12 months.
Suitable antibiotics before or after sex:
- Nitrofurantoin (1x50mg or 1x100mg)
- Fosfomycin (1x3000mg)
- Trimethoprim (1x100mg) => unfortunately, high resistance rates are now widespread
Suitable antibiotics for sustained intake (3-12 months long):
- Nitrofurantoin (1x100mg daily)
- Fosfomycin (3x3g weekly)
Once an antibiotic has been found that is tolerated by the body for long-term use, methenamine (Hiprex) is combined with a dose of 2x1g daily.
Links to articles about antibiotics: Antibiotics Natural Antibiotics
Methenamine is an antimicrobial medication for the treatment and prevention of urinary tract infections.
Taken orally (1g = 1 tablet, morning and evening), methenamine reaches the urine. In this slightly acidic environment, formalin (formaldehyde) is released. This has an antiseptic effect that inhibits bacterial growth and can therefore support the treatment of urinary tract infections. As the antibacterial activity of methenamine is greater in acidic urine, additional acidification of the urine may be necessary.
Methenamine is not licensed in Germany due to the potential carcinogenic formaldehyde content, hence it is also unavailable here. However, it can be purchased online, for example, in Denmark (trade name Haiprex) or England (trade name Hiprex).
In the private clinic on Harley Street 10 in London, treatment includes taking Hiprex together with antibiotics.
When talking about a biofilm, it means bacterial colonies that are shielded by an extracellular polymeric matrix (the biofilm) they produce themselves. The biofilm protects the bacteria from attacks of the immune system and the effects of antibiotics.
In a biofilm, the bacteria can survive in up to 1,500 times higher antibiotic concentrations, as it is difficult for the antibiotic to reach the bacteria. By taking antibiotics, the opposite effect may even occur: The biofilm formation is promoted because many antibiotics harm the protective microbiome (urobiome).
The English website Live UTI Free deals intensively with recurring urinary tract infections and describes the different stages of the life cycle of biofilms, Chronic Urinary Tract Infection vs. Recurrent UTI. It becomes clear and understandable why urinary tract infections recur.
Antibiotic in the form of long-term antibiotic therapy is still a means of choice for recurring HWI. The goal: When the biofilm breaks up in its life cycle and bacteria again enter the bladder, the antibiotic has a chance to fight the bacteria. The renewal of the entire bladder mucosa is a longer process (the lifespan of an urothelial cell can be up to 500 days), therefore the antibiotic must be taken for a longer period (at least 3 months, but usually longer).
More on biofilm inhibitors under Why does the antibiotic not work in acute urinary tract infections?
Nitrofurantoin is a chemotherapeutic agent from the antibiotic group of Nitrofurans and is used in the treatment of uncomplicated(!) urinary tract infections in adults.
- Sensitive against 86% of all pathogens causing uncomplicated cystitis.
- Only for uncomplicated cystitis (works only in the bladder, not in the tissue).
- Better effectiveness with acidic pH of urine.
- Longer antibiotic treatment (5 – 7 days) leads to better results.
- Not recommended for pregnant women in the third trimester (6th – 9th month).
- Not for kidney insufficiency.
- Pulmonary side effects (chronic pulmonary fibrosis, pulmonary edema, acute interstitial pneumonia) especially in older women after more than 12 months of long-term antibiotic treatment.
- => For long-term treatment, monitoring is necessary (lungs, liver, kidneys, nerves, blood).
Nitrofurantoin is a so-called prodrug. Prodrugs are substances that are administered to the patient in an inactive form and only later converted into an active substance in the human body. Nitrofurantoin is activated enzymatically in the bacteria themselves and then damages the bacterial DNA, proteins, and enzymes.
Nitrofurantoin is effective against most gram-positive and gram-negative bacteria that cause urinary tract infections (E. coli, Klebsiella, Enterococcus, Enterobacter, and Staphylococcus). According to resistance studies, Nitrofurantoin is sensitive to 86% of all pathogens causing uncomplicated cystitis. The risk of resistance formation is considered relatively low because the targets of the drug are so diverse.
However, there are two exceptions: Nitrofurans are naturally resistant to Pseudomonas aeruginosa and Proteus mirabilis (and related Providencia).
Nitro works only in the bladder
Antibacterial effective concentrations are only reached in the urine, and the active substance does not penetrate kidney tissue. Therefore, Nitrofurantoin (like Fosfomycin-Trometamol and Pivmecillinam) is only recommended for the treatment of uncomplicated cystitis and for prophylaxis in recurrent urinary tract infections. Nitrofurantoin is not suitable for pyelonephritis (UTI with fever, flank pain may indicate this).
Nitro likes it acidic
Nitrofurantoin works optimally when the pH of the urine is in the acidic range, which is why urine acidifying substances (e.g. ascorbic acid, methionine, methenamine/Hiprex®) are sometimes recommended. Alkalizing medications (or foods), such as Acetazolamide, Thiazides, may reduce the effectiveness of Nitrofurantoin.
Alternatives to Nitro
If Nitrofurantoin cannot be taken, the following alternatives are suitable as first-choice antibiotics for an acute uncomplicated urinary tract infection:
- Nitroxolin (Nitroxolin forte, Nilox® midi)
- Pivmecillinam (Selexid®, X-Systo®)
- Fosfomycin-Trometamol (Monuril®)
- Trimethoprim, only when local resistance rates are less than 20% (Selexid®, X-Systo®)
My Conclusion
Unfortunately, general practitioners still prescribe Nitrofurantoin somewhat hesitantly, even though it is a really effective and generally well-tolerated "antibiotic".
The classic side effects of broad-spectrum antibiotics (gastrointestinal issues => damaged microbiome) do not occur, as its effect is limited to the bladder.
Nitro covers almost all pathogens and is also suitable for long-term use in retarded form (macrocrystalline form) as a prophylactic treatment for recurrent bladder infections.
However, you really need to be careful about: The lung function should be monitored closely with prolonged use => I know several people who had to stop taking Nitro due to lung issues.
No, although Nitrofurantoin is effective against most gram-positive and gram-negative bacteria (in 86% of cases, such as E. coli, Klebsiella, Enterococcus, Enterobacter, and Staphylococcus).
Nitrofurans are naturally resistant to Pseudomonas aeruginosa and Proteus mirabilis (and the related Providencia).
Not effective against kidney involvement: Nitrofurantoin is very effective in the bladder, but it does not penetrate into the renal tissue (achieves no effective concentration). Therefore, if you have a urinary tract infection with fever and/or flank pain, Nitrofurantoin is not indicated.
No, Nitrofurantoin is prescription-only.
However, you don't necessarily need to visit a doctor's surgery to get a prescription. Since 2019, it has been permitted across the EU to obtain a prescription through online consultations.
In addition to Nitrofurantoin, there is another nitrofuran derivative called Furazidin, which is available without a prescription in Poland.
More information can be found under What antibiotics are available without a prescription for cystitis?
The antibacterial Furazidin, a Nitrofuran derivative, is similar to the better-known Nitrofurantoin and is available over-the-counter in Poland. The bacteriostatic mechanism of action (similar to Nitrofurantoin) works against both gram-positive (Staphylococcus epidermidis, Staphylococcus aureus, Staphylococcus faecalis) and gram-negative microorganisms (Enterobacteriaceae – Salmonella, Shygella, Proteus, Klebsiella, Escherichia, Enterobacter etc.) and is used to treat urinary tract, skin and soft tissue infections.
According to study, Nitrofurantoin superior
A 2018 study compared the effectiveness of Nitro and Furazidin against classical uropathogenic pathogens and multi-resistant strains of E. coli and Staphylococcus aureus. In vitro, Furazidin showed a better efficacy (Minimum inhibitory concentration) for the following pathogens:
- Proteus mirabilis
- Klebsiella pneumoniae
- MDR (= multi drug resistant) Staphylococcus aureus
- Escherichia coli
How to get it in the UK?
A successful order of UROFURAGINUM MAX 100 MG X 30 TABL could be placed on Apteka-Zielona.pl. It is a Polish online pharmacy registered in the national register, offering competitive prices compared to other online sellers.
Nitroxolin, like Nitrofurantoin, is used to treat acute and chronic urinary tract infections. It is listed in the S3 guideline as a first-choice antibiotic.
Nitroxolin has a broad spectrum of activity that covers numerous gram-negative and gram-positive bacterial species, including Mycoplasma hominis, Ureaplasma urealyticum (sexually transmitted organisms) and Candida spp. (fungi).
Resistance to the drug is rare, similar to Nitrofurantoin.
Like Nitrofurantoin, Nitroxolin requires an acidic environment for optimal efficacy (best at pH 5.5).
The key differences between Nitroxolin and Nitrofurantoin
- Different mode of action (inhibition of RNA polymerase in Nitroxolin, formation of DNA strand breaks in Nitrofurantoin)
- Nitroxolin is up to 64 times more active than Nitrofurantoin.
My Conclusion
If my infection was caused by Proteus mirabilis, Klebsiella pneumoniae or a multiresistant E. coli, I would definitely prefer Nitroxolin (unless contraindicated).
Fosfomycin (e.g. Monuril) is a true star among antibiotics. So far, very few bacteria are known to be resistant to Fosfomycin.
Fosfomycin inhibits an enzyme that the bacteria need for forming their cell wall, and this causes the bacteria to burst.
Since Fosfomycin is required for the treatment of severe, sometimes life-threatening infections, it should remain a last resort for uncomplicated urinary tract infections (the risk of developing resistance increases with frequent prescription).
It should therefore only be used when Nitrofurantoin, Pivmecillinam, or even Trimethoprim have failed to work, as the patient's symptoms suggest.
Therapy update
I frequently read that a single dose of Fosfomycin-Trometamol is not sufficient to cure cystitis. Also, there are cases where Fosfomycin-Trometamol does not seem to work effectively.
The University Clinic Vienna (Department of Infections and Tropics) has issued a therapy update "Acute Cystitis". It states that two doses of Fosfomycin-Trometamol, given 72 hours apart (not just a single shot), may be necessary to effectively treat cystitis.
- Two doses of Fosfomycin-Trometamol, spaced 72 hours apart, may be more effective than a single dose.
- Effectiveness of Fosfomycin-Trometamol in the urinary bladder model is highly variable.
- Development of resistance has been observed even in vivo studies.
- Individual variations in the absorption and distribution of the active substance in the body (pharmacokinetics).
- Need for further studies to determine the optimal dosage.
Fosfomycin is not a fluoroquinolone.
The fluoroquinolones (ciprofloxacin, levofloxacin, moxifloxacin, etc.) are another class of antibiotic, which belong to the broad-spectrum antibiotics and are considered reserve antibiotics, which should be used primarily in cases of complicated urinary tract infections. Not only because of their wide range of action, but also due to some serious side effects, fluoroquinolones should again be treated as reserve antibiotics.
Fosfomycin can either be administered via the bloodstream as an injection or taken orally. For oral administration, the active ingredient is present in powder or granule form as a combination with Trometamol. With the aid of Trometamol, the active ingredient Fosfomycin can be better absorbed in the gastrointestinal tract.
Fosfomycin-Trometamol is used to treat uncomplicated urinary tract infections, also preventively before surgical interventions on the urinary tract, or for long-term prophylaxis (every 10 days a single dose).
As the active ingredient continuously passes into the bladder through the bloodstream, Toilet visits should not be avoided even shortly after taking Fosfomycin, but are actually beneficial for recovery.
Contraindications/Interactions related to the digestive system:
- Diarrhoea, Vomiting: If you have severe diarrhoea or frequent vomiting, the active ingredient may not reach sufficient levels in the bloodstream.
- Gastric motility: Substances that promote rapid movement of stomach and intestinal contents (e.g. for preventing nausea and vomiting) can affect the absorption of Fosfomycin into the body (e.g. Metoclopramide, Domperidone)
Five days of Nitrofurantoin is superior to a single dose of Fosfomycin, according to the study.
Both Nitrofurantoin and the once-daily Fosfomycin are frequently prescribed for uncomplicated cystitis.
In a multinational study with 513 women (from Switzerland, Poland, and Israel), the two antibiotics were compared: Three times daily 100mg Nitrofurantoin for five days versus a single dose of 3000mg Fosfomycin.
The result: Twenty-eight days after completing treatment, 70% of the Nitrofurantoin group were symptom-free, whereas in the Fosfomycin group, only 58% were symptom-free. Furthermore, in the urine culture, the causative germ was not detectable in 74% of the Nitrofurantoin group, compared to 63% of the Fosfomycin group.
It is suspected that Fosfomycin may be less effective than Nitrofurantoin because widespread use has led to the development of resistance among pathogens.
Fosfomycin single dose may not be sufficient: New studies on the efficacy of a single dose of 3000mg Fosfomycin suggest that this is an insufficient dose, and might even promote resistance. Fosfomycin is a reserve antibiotic: Its broad-spectrum effect is urgently needed for use against multiresistant pathogens, which requires a more cautious approach.
A possible treatment approach: For example, administering 3000mg Fosfomycin every three days for three, six, or even nine days.
As a general rule: The sensitivity of pathogens decreases as antibiotic use increases.
The Problem of Multiresistance
Antibiotics inhibit the growth of bacteria through a variety of different mechanisms (bacteriostatic) or kill them (bactericidal).
BUT: The more frequently bacteria are exposed to a particular antibiotic, the higher the likelihood that they will become resistant to it, rendering the medication ineffective. The problem becomes more serious when a bacterium develops resistance to multiple antibiotics - this is referred to as multidrug-resistant pathogens (e.g. MRSA - methicillin-resistant Staphylococcus aureus), which are difficult to treat.
Once bacteria have developed resistance mechanisms, they can transfer them to another bacterial species (via mobile genetic elements called plasmids). This results in entire bacterial strains becoming resistant to antibiotics and potentially spreading (especially feared in hospitals => "hospital-acquired pathogens").
Why do Antibiotic Resistances Develop?
Antibiotic resistances primarily arise because antibiotics are not used correctly:
- too frequently
- at too low a dose
- for too long (yes, exactly, too long is the problem, because bacteria have more time to develop resistance)
- unnecessarily (e.g. for viral infections)
- careless use in intensive animal farming
As short as possible, as long as necessary
Depending on the severity of the disease, antibiotics should only be used for as short a time as possible (but as long as necessary), as the risk of developing resistance increases with the duration of use.
What can you contribute?
Antibiotic-resistant bacteria pose a danger to us all, as they cause infections that are difficult to treat. If we repeatedly take antibiotics unnecessarily or incorrectly, we contribute to the rise of antibiotic-resistant bacteria, one of the world's greatest health problems.
Do your part by
- questioning every antibiotic use => many uncomplicated UTIs heal without antibiotics
- insisting on a urine culture with antibiotic susceptibility testing => this is the only way to choose the best antibiotic
- not taking reserve antibiotics unnecessarily (e.g. fluoroquinolones)
- strictly following the prescription and taking the antibiotics exactly as directed
- only taking antibiotics prescribed by a doctor => self-medication with antibiotics is not responsible!
Post-antibiotic era 2030
The WHO (World Health Organization) warns that we are heading for an era where antibiotics may only be partially effective or not work at all against bacteria. To counter this, more effort is needed in antibiotic research, and at the same time, the use of antibiotic therapy must become more careful.
For Antibiotic Stewardship (rational and responsible use of antibiotics) to prevail, further education for medical professionals is obviously necessary. According to Statista, the knowledge of European medical professionals regarding antibiotic resistance is quite concerning.
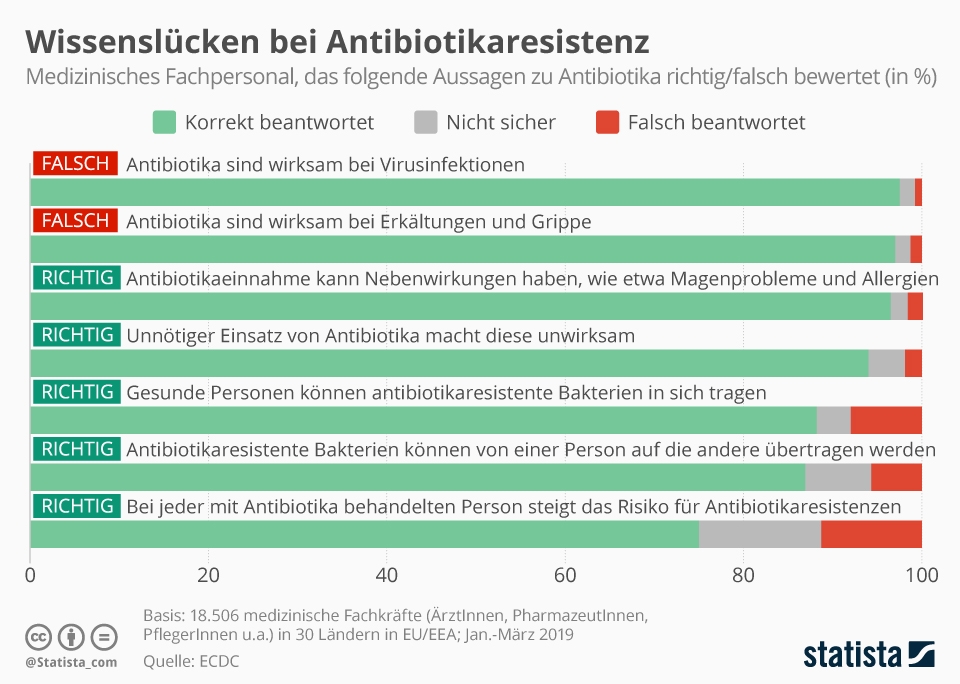
Resistance Mechanisms
First of all, it is important to know that there are two types of resistance mechanisms: natural or acquired resistance.
Natural resistance means that an antibiotic simply cannot work against a germ because, for example, the target site is absent. An example: Mycoplasmas (sexually transmitted) do not have a cell wall => therefore, antibiotics that inhibit cell wall synthesis (e.g. penicillins, fosfomycin) are ineffective. There are other reasons for natural resistance: the antibiotic may either not penetrate the lipid membrane of Gram-negative bacteria or it is immediately pumped out by the bacterium.
Specific examples of natural/intrinsic resistance:
- Proteus mirabilis and Pseudomonas aeruginosa are naturally resistant to nitrofurans.
- Penicillin resistance in Gram-negative bacteria (e.g. E. coli).
- Staphylococcus saprophyticus is intrinsically resistant to Mecillinam (Selexid®, Pivmelam®, X-Systo®).
Acquired resistance means that a bacterium has developed a mechanism that makes one or more antibiotics ineffective.
This phenomenon can also arise naturally => genes can mutate randomly during reproduction, and this may give a bacterium "accidental" resistance.
A much more common cause of acquired resistance is the transfer of genetic material: Bacteria exchange parts of their genetic material (=genes) via so-called resistance plasmids. In this way, a bacterium with resistant properties can pass on its "tool" to another, making the bacteria insensitive to an antibiotic.
Less frequently, genetic material is transferred via viruses (phages) (e.g. penicillin resistance in Staphylococcus aureus through phage transduction).
Irresponsible Use of Antibiotics = Selection Pressure = Resistance
Resistance is an inevitable evolutionary process through mutation and selection. Antibiotics create the selection pressure that promotes the growth of resistant germs.
What is meant by selection pressure? Selection pressure is actually a normal event in nature. It ensures that the "strong" survive and the "weak" perish.
When antibiotics are used, resistant bacteria have an advantage over non-resistant bacteria. While the "harmless" ones are killed or inhibited, the "tough" ones (resistant bacteria) can survive the antibiotic treatment and continue to multiply and spread.
=> The higher the selection pressure (usually antibiotics), the more resistance mechanisms a germ acquires.
If you want to delve further into the topic of antibiotics and resistance, I can recommend the materials from a Swiss symposium on the topic of Infectiology and Hygiene in the Perioperative Setting.
Multidrug-Resistant Pathogens
Multidrug resistance is present when only one or no antibiotic group is still sensitive.
In most cases, this involves an ESBL-producing pathogen. ESBL bacteria ("Extended Beta-Lactamase" or "Beta-lactamase with extended spectrum") can split the beta-lactamase rings of significant antibiotic classes with an enzyme, rendering them ineffective (penicillins, cephalosporins of all generations, and monobactams). These enzymes are most commonly found in typical UTI pathogens such as Escherichia coli and Klebsiella.
ESBL-producing bacteria colonise the intestines. For healthy individuals, the colonisation is usually symptom-free and harmless. However, there is a risk that the resistant intestinal bacteria could spread to other parts of the body, such as the urinary tract.
Multidrug-resistant pathogens (MDR) are especially prevalent in countries with very high antibiotic consumption (e.g. in the Middle East). The high transmission rate of multidrug-resistant pathogens is particularly problematic. Some studies show that, for example, one third of Germans who have travelled to countries with high resistance rates return with an MDR. Among returnees from India, this figure rises to up to 70 percent.
MRSA, EBL & Co
The most important antibiotic-resistant pathogens:
- MRSA (Methicillin-resistant Staphylococcus aureus) => Staphylococcus aureus
- ESBL (Extended-Spectrum Beta-Lactamases) => Escherichia coli, Klebsiella pneumoniae, Proteus mirabilis
- MRGN (multidrug-resistant gram-negative pathogens) => Escherichia coli and Klebsiella pneumoniae, Pseudomonas aeruginosa
- VRE (Vancomycin-resistant Enterococci) => Enterococcus faecium and Enterococcus faecalis
Behind these abbreviations are dangerous pathogens, against which hardly any antibiotics are effective anymore. A growing problem are ESBL-producing bacteria. They deactivate almost all beta-lactams and are not inhibited by Tazobactam or Clavulanic acid.
Avoiding Resistances
If microbes are exposed to suboptimal antibiotic concentrations for an extended period of time, they develop resistance. For this reason, bacteria should be targeted with a high antibiotic dose over the shortest possible time. This contradicts the treatment option of long-term antibiotic therapy for recurrent urinary tract infections, but it is often the last resort for those affected. Regarding the dosage of long-term antibiotics, recommendations differ within Europe: While in Germany, for example, delayed-release Nitrofurantoin is administered at a low dose, in England, it is also used at a normal to high dose over a longer period.
There are a number of measures to avoid resistance: In Switzerland, the project "StAR" (Strategy Antibiotic Resistance) aims to counteract the looming multiresistance crisis. The goal is to ensure the long-term effectiveness of antibiotics for both humans and animals . This not only focuses on the rational use of antibiotics in humans but also addresses the use of antibiotics in agriculture and the spread of excreted antibiotics/MRE in the environment (e.g. in wastewater). Another key area of action: Research & Development => How can proven antibiotics be improved regarding resistance? How can we find new active substances that crack the protective shell (= outer membrane) of bacteria? For information for both healthcare professionals and patients, another website has been created: https://www.antibiotika-richtig-einsetzen.ch/ . It is definitely worth checking out.
Risk of Infection in Hospitals: Every urethra is colonized by all kinds of pathogens, and when a catheter is inserted into the urethra, they can travel up to the bladder or even the kidneys, causing infections.
For more on the topic of resistance avoidance, see What happens when you take unnecessary antibiotics?
Recognising and Treating Resistant Pathogens
Depending on how resistant the pathogens are to antibiotics, treating the infection can become difficult to impossible.
Uncomplicated cystitis with ESBL-producing bacteria can be treated with Nitrofurantoin or Cotrimoxazole.
MRSA: Fosfomycin is used in combination with Vancomycin to treat infections caused by MRSA.
Ideally, along with the diagnosis of "ESBL-producing pathogen" or MRSA, an antibiogram is also available, which should always serve as the basis for targeted antibiotic therapy.
Resistance Situation
- Trimethoprim 22.0%
- Trimethoprim + Sulfamethoxazole 21.4%
- Pivmecillinam 3.0%
- Fosfomycin-Trometamol 0.8%
- Nitrofurantoin 0.4%
The resistance rate against Nitrofurantoin remains consistently below 4.5% in countries where it is frequently used to treat urinary tract infections. No correlation between the use of Nitrofurantoin and increased occurrences of ESBL, MRSA, or VRE has been reported.
Ciprofloxacin therapy increases the risk of colonisation with a CIP-resistant strain after 28 days => with effects on household members.
For a detailed graphical representation of the resistance situation by country, pathogens, and antibiotics on a timeline, I recommend the Resistance Map.
For a detailed report on the resistance situation in Europe 2022, I recommend the document Antimicrobial resistance surveillance in Europe 2022.
Antibiotic resistance is increasing at an alarming rate worldwide. Multiresistant bacteria continue to cause major problems in hospitals.
Alternative treatment options are urgently needed.
Mustard oils for problematic pathogens
Mustard oils (e.g. Angocin®) are recommended as a treatment option when resistant pathogens are detected.
According to various in vitro studies, mustard oils show a broad antibacterial spectrum (both in gram-positive and gram-negative ranges), even against resistant forms of E. coli and problem pathogens such as MRSA. You can find more information in my article Natural Antibiotic .
Bacteriophages - the "good" viruses
Phages are viruses that rely on bacteria as host organisms for reproduction. When a phage finds a suitable host (bacterium), it attaches to it and forces the host to replicate the phage's genetic material inside. New phages are produced and, after the bursting of the bacterium, released. The bacterium is destroyed, and many new phages seek out bacteria to destroy.
The remarkable thing: Bacteriophages are specialized in specific bacteria, meaning they act very specifically on the bacteria they can kill. In contrast to broad-spectrum antibiotics that kill a variety of bacterial strains.
Another advantage: Bacteriophages multiply at the site of infection, as long as bacteria are present. Once there are no more bacteria, the phages are gone as well.
Advantage = Disadvantage: Bacteriophages must exactly match the bacterial pathogen, otherwise, they will ignore it and the infection will not be treated. Therefore, the exact pathogen causing the infection must first be determined (e.g. via a urine culture). Only then can it be checked which phages are effective.
In Eastern European countries such as Georgia, phage therapy has been used for much longer, and large databases of bacteria and phages already exist there. Currently, there is no approval for phages in this country – the requirements in terms of quality and safety have not yet been sufficiently proven (e.g. through randomized controlled clinical trials).
My conclusion: In the Facebook support group Embedded Bladder Infection Help and Exchange there are some women who have successfully fought their recurring (embedded) bladder infections with bacteriophages after a long suffering journey. The process is not as straightforward as an antibiotic treatment. First, a urine sample must be sent to a clinic in Georgia (e.g. the hospital in Tbilisi). There, the pathogens are isolated, and the right phages are found. The phages, in the form of tablets and vaginal suppositories, are then sent back to you by post. The therapy lasts about 3 months.